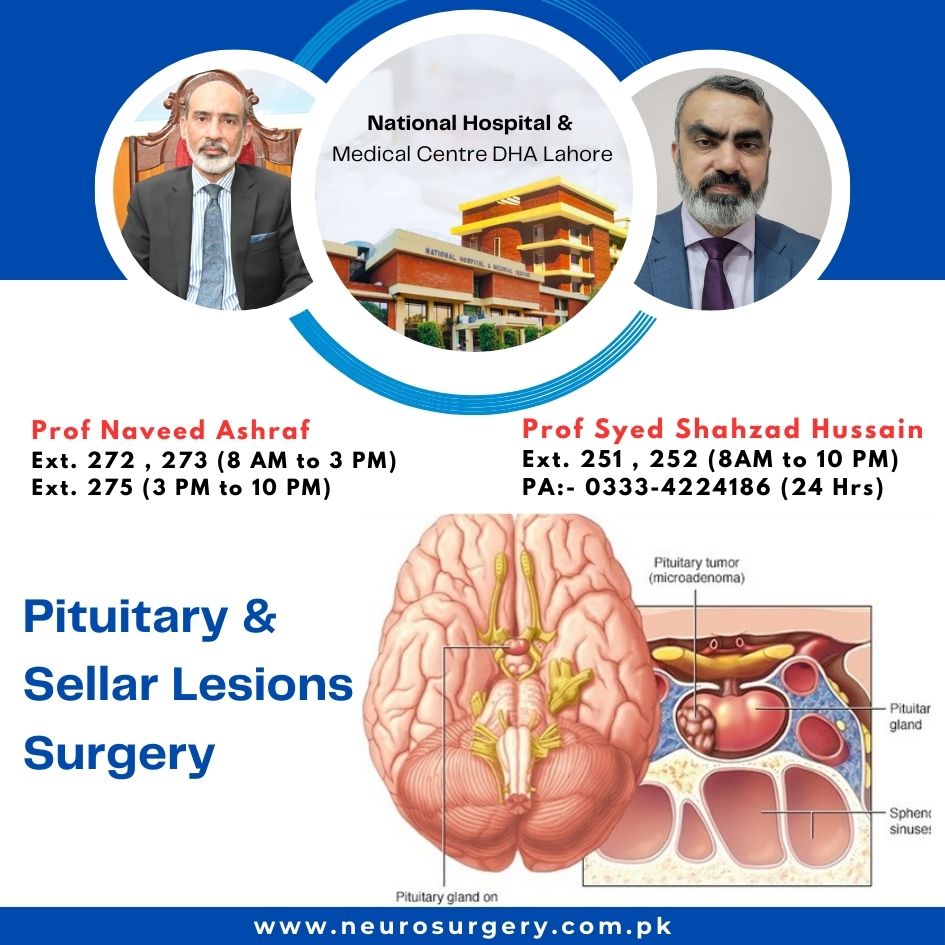
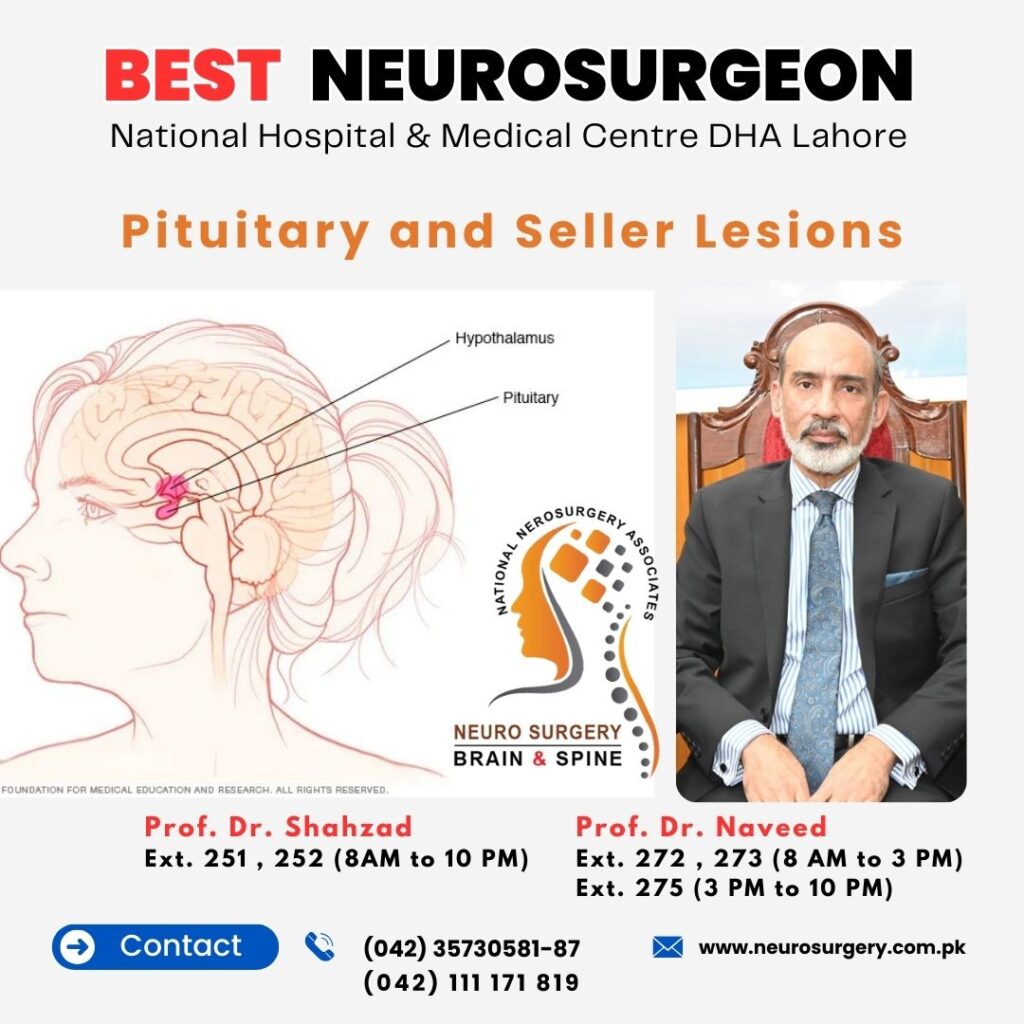
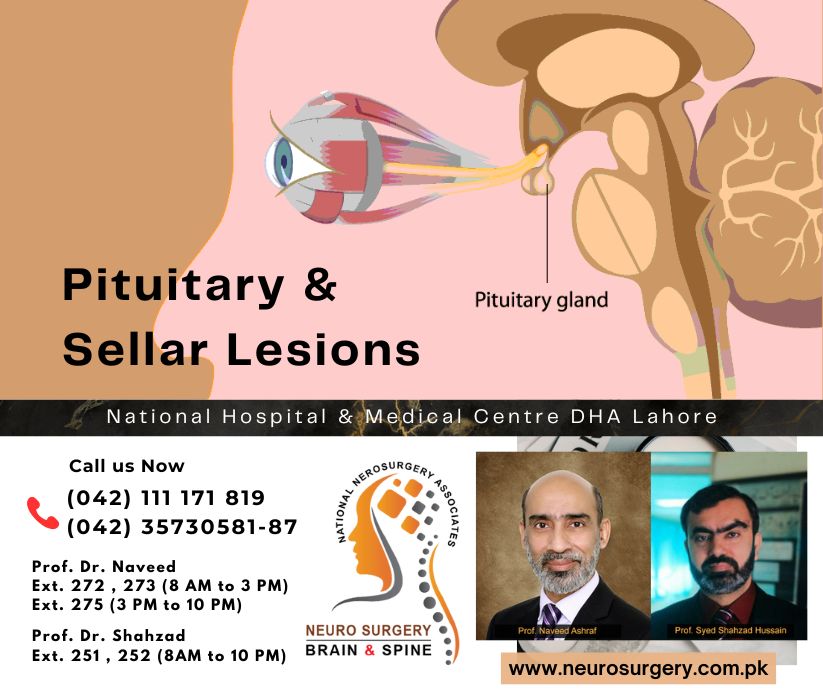
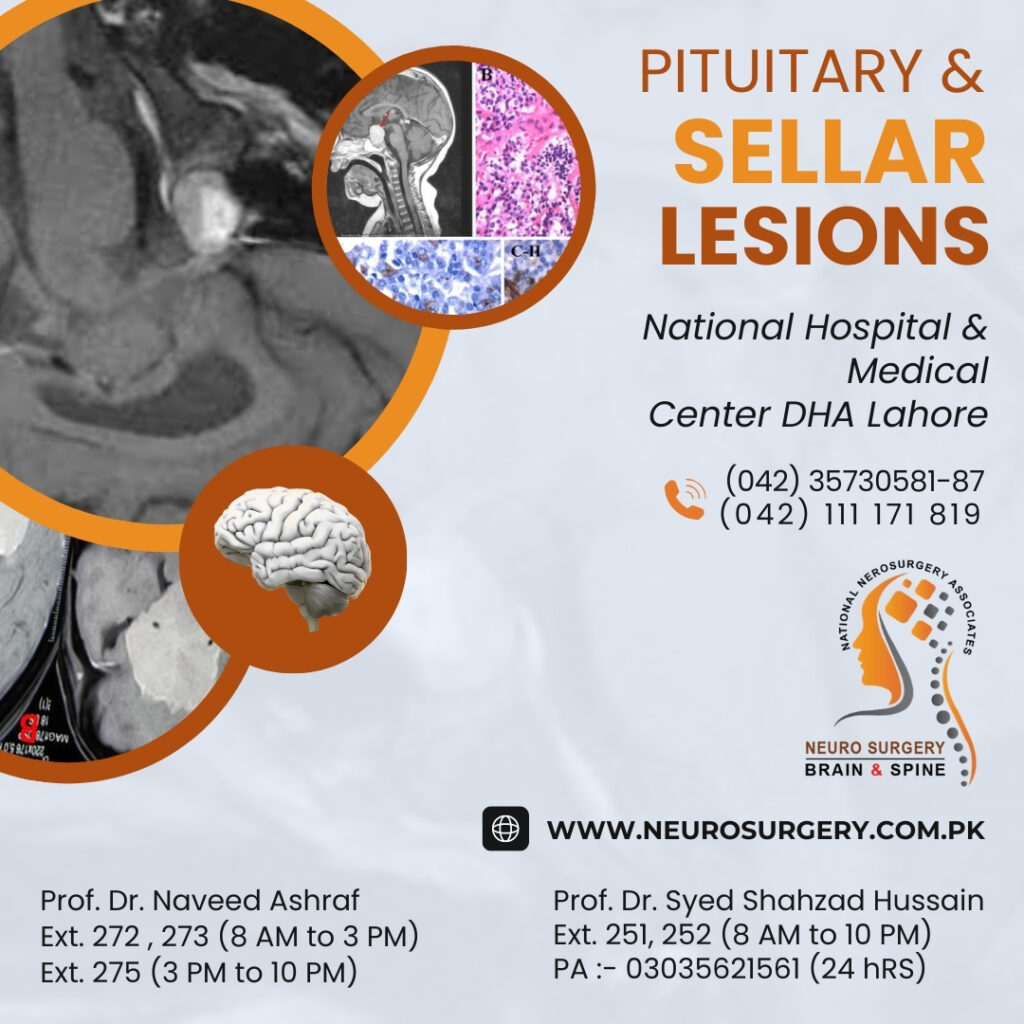
Pituitary and Sellar Lesions
The *pituitary gland*, located in the **sella turcica is a critical endocrine organ that regulates hormones controlling growth, metabolism, reproduction, and stress response. It is further controlled by releasing or inhibitory hormones from Hypothalamus. Pituitary gland has two lobes anterior and posterior lobe. There are 6 hormones that release from anterior lobe and 2 from posterior lobe.
*Sellar Lesions* can arise from the pituitary itself or surrounding structures and may cause hormonal dysfunction (excess secretion or deficiency) or local mass effects leading to visual impairment, cranial nerve palsies, hydrocephalus, stroke.
Types of Pituitary / Sellar Lesions
1. Pituitary Adenomas (Most Common)
– Benign tumors of pituitary cells, classified by:
– Size:
- Microadenoma* (<1 cm)
- Macroadenoma* (≥1cm)
- Hormone secretion
- Functional (secreting) adenomas that secrete active hormones like prolactinoma
- Non-functional (non-secreting): they usually cause symptoma due to mass effect. Mostly patients remain asymptomatic till adenoma acheive a certain size and causes mass effect.
- Classification on the basis of electron microscopy *
– On the basis of light microscopy
| Type | Hormone Excess | Clinical Features |
|---|---|---|
| Prolactinoma | Prolactin | Galactorrhea, secondary amenorrhea, infertility, erectile dysfunction (ED) |
| Somatotroph | GH (Growth Hormone) | Acromegaly (adults), gigantism (children) |
| Corticotroph | ACTH | Cushing’s disease (central obesity, moon face, striae) |
| Thyrotroph | TSH | Secondary hyperthyroidism (rare) |
| Gonadotroph | FSH / LH | Usually non-functional (mass effects) |
Non-Functional Adenomas
Non-functional pituitary adenomas do not secrete biologically active hormones. They usually present with mass effects, which include:
-
Headaches – due to stretching of the dura
-
Visual field defects – classically bitemporal hemianopia from compression of the optic chiasm
-
Hypopituitarism – compression of normal pituitary tissue leading to ↓ ACTH, TSH, FSH/LH, GH
-
Cranial nerve palsies – involving CN III, IV, VI if the cavernous sinus is affected
-
Hydrocephalus – caused by suprasellar extension and compression of the third ventricle
2. Craniopharyngioma
-
Nature: Benign, slow-growing cystic or solid tumor, arising from remnants of Rathke’s pouch
-
Epidemiology: Most common in children and young adults
-
Types:
-
Adamantinomatous – more common in children
-
Papillary – usually seen in adults
-
Clinical Features (Symptoms):
-
Headache
-
Visual impairment – due to compression of the optic chiasm
-
Endocrine dysfunction:
-
Growth failure in children
-
Hypothyroidism
-
ADH deficiency → Diabetes insipidus
-
Hypogonadism
-
3. Rathke’s Cleft Cyst
-
Benign, fluid-filled cyst arising from remnant of Rathke’s pouch
-
Often asymptomatic, but when symptomatic, it may mimic pituitary adenoma or craniopharyngioma
4. Meningioma
-
Arises from sellar/parasellar meninges
-
Slow-growing, compresses pituitary & optic structures
5. Pituitary Apoplexy
-
Sudden hemorrhage or infarction of a pituitary adenoma (or sometimes normal pituitary) → causes acute neurological or endocrine dysfunction
-
Medical Emergency!
-
Symptoms:
-
Severe headache (thunderclap onset)
-
Vision loss (optic nerve/chiasm compression)
-
Ophthalmoplegia (cranial nerves III, IV, VI palsy)
-
Hypotension (ACTH deficiency → adrenal crisis)
-
-
Treatment:
-
High-dose glucocorticoids (IV hydrocortisone)
-
Endoscopic transsphenoidal decompression in many cases
-
6. Metastasis to Pituitary
-
Rare, but can occur from breast, lung, prostate cancers
7. Aneurysm / Inflammatory Lesions
-
Can mimic pituitary masses
-
Examples: Inflammation (hypophysitis)
Diagnosis of Sellar Lesions
1. Pituitary Hormonal Workup
(to assess hypersecretion or deficiency)
-
Prolactin
-
IGF-1 (GH)
-
ACTH / Cortisol
-
TSH / Free T4
-
FSH / LH
-
Testosterone / Estradiol
2. Imaging
-
MRI brain with pituitary protocol (gold standard)
-
Dynamic MRI brain (Pituitary gland) – most useful in detecting microadenomas
-
CT brain / CT angiogram – for surgical planning (e.g., visualization of sphenoid sinus pneumatization, detection of calcifications, pituitary apoplexy, or aneurysms)
3. Visual Field Testing
Treatment Approaches
| Lesion | Management |
|---|---|
| Prolactinoma | Dopamine agonists (cabergoline, bromocriptine); surgical excision in selected cases |
| Other Functional Adenomas | Surgery – Endoscopic transsphenoidal or Transcranial approach |
| Non-Functional Adenoma | Surgery is the mainstay of treatment, especially if the patient is symptomatic |